That's exactly what I did, and if you do so using the number ranges shown in my post, you get what I showed in my post: a bell curve.You didn't even count the data points correctly. All you gotta do is copy/paste to spreadsheet, sort them in order and highlight all in said range to get an accurate count.
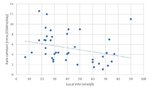
You do not create a histogram with different sized bins, nor by further biasing your histogram by selecting the bin values on the basis of something you think you've seen and want to make a point of. The fact you are trying to make this argument demonstrates nothing other than that you do not understand histograms and that you do not treat the data neutrally.
This is without considering that you don't necessarily expect a "perfect" bell curve anyway, especially with limited data points, because of random fluctuation. (In much the same way if you roll a conventional die 42 times, you are deeply unlikely to end up with exactly 7 instances of each number 1-6)
They aren't "right on the 2.5 line". They are spread across a region of ~2-3. They appear "on the 2.5 line" because of the wider scale. This, again, is why we subject things to analysis rather than rely on someone's visual approximation.I wonder why a quarter of the studies are right on the 2.5 line that CPG stated as their average...
Yes, but why are you pointing this out? I have repeatedly said many times that government guidance states that there are "at-risk" groups and advises them to take more or to follow specific medical guidance. This has been answered so often it is akin to banging one's head against a wall.And outside of young kids, about a quarter have levels 25 nmol or below. Just saying.
Yes, doctors do not exist in their own bubbles. Guidelines exist at all levels and individual institutions may well decide treatments in line with or different from government guidelines according to their own systems: often likely to be consensus of their senior staff. The reason they do so is not so much government guidelines, but the threat of being sued for malpractice, and that doctors should work in teams and have oversight rather than let loose cannons be dictators of their own little empire. If a doctor wishes to protest his institution's treatment plan, he should take it up with the institution through their normal processes, rather than embarrass them by going to a political debate and saying they won't let him save people's lives.Kory resigned and went to another place. Maybe he got in trouble vs his choice. I'd hardly call him most likely still making a great salary somewhere else "getting in trouble". This isn't the 1st I've heard of institutions being an issue with treatment. One private practice doctor said he was very fortunate to have a private practice so he could treat how he saw fit. Yes, technically doctors can prescribe whatever they want, but that's not how it always goes down either.
The concept of the "maverick surgeon" who flouts the system to save his patients is a well-worn trope, and so frequently used because it's attractive, an underdog story of the little guy overcoming the senseless, faceless, stupid, sclerotic authority. The unfortunate reality is nine times out of ten the "maverick surgeon" is actually a danger to his patients. The same people lionising the maverick hero surgeon rage at why the system wasn't more restrictive to the maverick villain surgeons, seemingly not realising the two are mutually contradictory visions of how the system should work.